GLAUCOMA
Glaucoma is a disease in which the optic nerve is damaged, leading to progressive, irreversible loss of vision. It is often, but not always, associated with increased pressure of the fluid in the eye.
The nerve damage involves loss of retinal ganglion cells in a characteristic pattern. There are many different sub-types of glaucoma but they can all be considered a type of optic neuropathy. Raised intraocular pressure is a significant risk factor for developing glaucoma (above 21 mmHg or 2.8 kPa). One person may develop nerve damage at a relatively low pressure, while another person may have high eye pressure for years and yet never develop damage. Untreated glaucoma leads to permanent damage of the optic nerve and resultant visual field loss, which can progress to blindness.
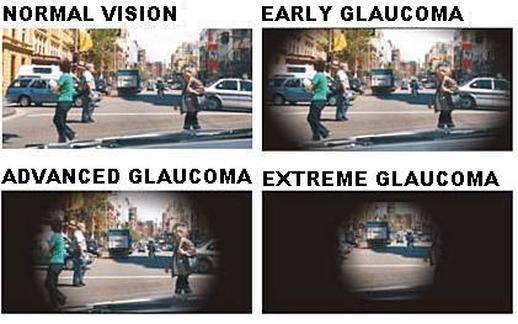
Glaucoma has been nicknamed the "silent thief of sight" because the loss of vision normally occurs gradually over a long period of time and is often only recognized when the disease is quite advanced. Once lost, this damaged visual field cannot be recovered. Worldwide, it is the second leading cause of blindness.
The nerve damage involves loss of retinal ganglion cells in a characteristic pattern. There are many different sub-types of glaucoma but they can all be considered a type of optic neuropathy. Raised intraocular pressure is a significant risk factor for developing glaucoma (above 21 mmHg or 2.8 kPa). One person may develop nerve damage at a relatively low pressure, while another person may have high eye pressure for years and yet never develop damage. Untreated glaucoma leads to permanent damage of the optic nerve and resultant visual field loss, which can progress to blindness.
Glaucoma has been nicknamed the "silent thief of sight" because the loss of vision normally occurs gradually over a long period of time and is often only recognized when the disease is quite advanced. Once lost, this damaged visual field cannot be recovered. Worldwide, it is the second leading cause of blindness.
Glaucoma affects 1 in 100 people aged fifty and younger, and 1 in 10 over the age of eighty. If the condition is detected early enough it is possible to arrest the development or slow the progression with medical and surgical means. Anyone can develop glaucoma however a person is at higher risk if any of the following are present:-
• Increased intraocular pressure within the eye
• Age – over 40 years (especially over 60 years)
• Family history
• African heritage
• Hispanic heritage
• Central corneal thickness less than 0.5 mm
• History of migraines
• Myopia (short sightedness)
• Diabetes
• Steroid use
• Diabetes
• Hypertension
• Eye Injury
• Increased intraocular pressure within the eye
• Age – over 40 years (especially over 60 years)
• Family history
• African heritage
• Hispanic heritage
• Central corneal thickness less than 0.5 mm
• History of migraines
• Myopia (short sightedness)
• Diabetes
• Steroid use
• Diabetes
• Hypertension
• Eye Injury
African Heritage
While glaucoma symptoms vary among black populations in different international regions, glaucoma clearly affects those of African heritage more. It is six to eight times more common in African than in Caucasians making glaucoma the leading cause of blindness among African. In addition to this higher frequency, glaucoma often occurs earlier in life in African heritage on average, about 10 years earlier than in other ethnic populations.
The reasons for the higher rate of glaucoma and subsequent blindness among African heritage are still unknown. However, researchers are becoming more and more certain that African heritage are genetically more likely to be susceptible to glaucoma, making early detection and treatment all the more important. For example, there may be a greater susceptibility to optic nerve damage, which causes vision loss, for blacks with glaucoma.
In African heritage, glaucoma generally occurs earlier which may need a lower target eye pressure and earlier extensive tests than other population groups. Initial results from the Advanced Glaucoma Intervention Study (AGIS) show that ethnicity may also be a factor in determining the better surgical treatment for glaucoma. Initially expecting both blacks and whites to have similar responses, researchers found that black patients with advanced glaucoma responded better to laser surgery than filtering (cutting) surgery. Now, an eye doctor’s recommendation for surgery may consider the patient’s race in addition to other important aspects of their individual health.
It is important to note, however, that treatments cannot be generalized. Each patient, regardless of race, should continue to be evaluated on the individual state of his or her disease, with a target pressure and treatment plan unique to each patient.
Early diagnosis and treatment is key in preventing vision loss from glaucoma. It is recommended that African heritage groups get a thorough check for glaucoma every one to two years after age 35.
People Over 60
Glaucoma is much more common among older people. You are six times more likely to get glaucoma if you are over 60 years old.
Family Members with Glaucoma
The most common type of glaucoma, primary open-angle glaucoma, is hereditary. If members of your immediate family have glaucoma, you are at a much higher risk than the rest of the population. Family history increases risk of glaucoma four to nine times.
Hispanics in Older Age Groups
Recent studies indicate that the risk for Hispanic populations is greater than those of predominantly European ancestry, and that the risk increases among Hispanics over age 60.
Asians
People of Asian descent appear to be at some risk for angle-closure glaucoma. Angle-closure glaucoma accounts for less than 10% of all diagnosed cases of glaucoma. Otherwise there is no known increased risk in Asian populations.
Steroid Users
Some evidence links steroid use to glaucoma. A study reported in the Journal of American Medical Association, March 5, 1997, demonstrated a 40% increase in the incidence of ocular hypertension and open-angle glaucoma in adults who require approximately 14 to 35 puffs of steroid inhaler to control asthma. This is a very high dose, only required in cases of severe asthma.
Eye Injury
Injury to the eye may cause secondary open-angle glaucoma. This type of glaucoma can occur immediately after the injury or years later.
Blunt injuries that “bruise” the eye (called blunt trauma) or injuries that penetrate the eye can damage the eye’s drainage system, leading to traumatic glaucoma. The most common cause is sports-related injuries such as baseball or boxing.
Read more about traumatic glaucoma.
While glaucoma symptoms vary among black populations in different international regions, glaucoma clearly affects those of African heritage more. It is six to eight times more common in African than in Caucasians making glaucoma the leading cause of blindness among African. In addition to this higher frequency, glaucoma often occurs earlier in life in African heritage on average, about 10 years earlier than in other ethnic populations.
The reasons for the higher rate of glaucoma and subsequent blindness among African heritage are still unknown. However, researchers are becoming more and more certain that African heritage are genetically more likely to be susceptible to glaucoma, making early detection and treatment all the more important. For example, there may be a greater susceptibility to optic nerve damage, which causes vision loss, for blacks with glaucoma.
In African heritage, glaucoma generally occurs earlier which may need a lower target eye pressure and earlier extensive tests than other population groups. Initial results from the Advanced Glaucoma Intervention Study (AGIS) show that ethnicity may also be a factor in determining the better surgical treatment for glaucoma. Initially expecting both blacks and whites to have similar responses, researchers found that black patients with advanced glaucoma responded better to laser surgery than filtering (cutting) surgery. Now, an eye doctor’s recommendation for surgery may consider the patient’s race in addition to other important aspects of their individual health.
It is important to note, however, that treatments cannot be generalized. Each patient, regardless of race, should continue to be evaluated on the individual state of his or her disease, with a target pressure and treatment plan unique to each patient.
Early diagnosis and treatment is key in preventing vision loss from glaucoma. It is recommended that African heritage groups get a thorough check for glaucoma every one to two years after age 35.
People Over 60
Glaucoma is much more common among older people. You are six times more likely to get glaucoma if you are over 60 years old.
Family Members with Glaucoma
The most common type of glaucoma, primary open-angle glaucoma, is hereditary. If members of your immediate family have glaucoma, you are at a much higher risk than the rest of the population. Family history increases risk of glaucoma four to nine times.
Hispanics in Older Age Groups
Recent studies indicate that the risk for Hispanic populations is greater than those of predominantly European ancestry, and that the risk increases among Hispanics over age 60.
Asians
People of Asian descent appear to be at some risk for angle-closure glaucoma. Angle-closure glaucoma accounts for less than 10% of all diagnosed cases of glaucoma. Otherwise there is no known increased risk in Asian populations.
Steroid Users
Some evidence links steroid use to glaucoma. A study reported in the Journal of American Medical Association, March 5, 1997, demonstrated a 40% increase in the incidence of ocular hypertension and open-angle glaucoma in adults who require approximately 14 to 35 puffs of steroid inhaler to control asthma. This is a very high dose, only required in cases of severe asthma.
Eye Injury
Injury to the eye may cause secondary open-angle glaucoma. This type of glaucoma can occur immediately after the injury or years later.
Blunt injuries that “bruise” the eye (called blunt trauma) or injuries that penetrate the eye can damage the eye’s drainage system, leading to traumatic glaucoma. The most common cause is sports-related injuries such as baseball or boxing.
Read more about traumatic glaucoma.
TYPES OF GLAUCOMA
1. Primary open-angle Glaucoma
This is the most common form of glaucoma. It happens when the eye’s drainage canals become clogged over time. The inner eye pressure (also called intraocular pressure or IOP) rises because the correct amount of fluid can’t drain out of the eye. With open-angle glaucoma, the entrances to the drainage canals are clear and should be working correctly. The clogging problem occurs further inside the drainage canals, similar to a clogged pipe below the drain in a sink.
Most people have no symptoms and no early warning signs. If open-angle glaucoma is not diagnosed and treated, it can cause a gradual loss of vision. This type of glaucoma develops slowly and sometimes without noticeable sight loss for many years. It usually responds well to medication, especially if caught early and treated.
This is the most common form of glaucoma. It happens when the eye’s drainage canals become clogged over time. The inner eye pressure (also called intraocular pressure or IOP) rises because the correct amount of fluid can’t drain out of the eye. With open-angle glaucoma, the entrances to the drainage canals are clear and should be working correctly. The clogging problem occurs further inside the drainage canals, similar to a clogged pipe below the drain in a sink.
Most people have no symptoms and no early warning signs. If open-angle glaucoma is not diagnosed and treated, it can cause a gradual loss of vision. This type of glaucoma develops slowly and sometimes without noticeable sight loss for many years. It usually responds well to medication, especially if caught early and treated.
2. Angle-closure Glaucoma
This happens when the drainage canals get blocked or covered over, like a sink with something covering the drain. This is relatively uncommon type of glaucoma, which causes pain, blurring of vision and a red eye. Sometimes people may notice halos around street lights. This condition tends to occur over 24-48 hours, due to a very rapid rise in the eye pressure. Early treatment can reverse the problem and prevent long-term visual damage. This type of glaucoma is also known as acute glaucoma or narrow angle glaucoma.
With angle-closure glaucoma, the iris is not as wide and open as it should be. The outer edge of the iris bunches up over the drainage canals, when the pupil enlarges too much or too quickly. This can happen when entering a dark room.
A simple test can be used to see if your angle is normal and wide or abnormal and narrow. Treatment of angle-closure glaucoma usually involves surgery to remove a small portion of the outer edge of the iris. This helps unblock the drainage canals so that the extra fluid can drain. Usually surgery is successful and long lasting. However, you should still receive regular check-ups. Symptoms of angle-closure glaucoma may include headaches, eye pain, nausea, rainbows around lights at night, and very blurred vision.
3. Normal Tension Glaucoma (NTG)
Normal tension glaucoma (NTG) is also known as low-tension glaucoma or normal pressure glaucoma. In this type of glaucoma, the optic nerve is damaged even though intraocular pressure (IOP) is not very high. Doctors do not know why some people’s optic nerves suffer damage even though pressure levels are in the “normal” range (between 10-20 mm Hg). In fact, about 20% of all glaucoma patients have this form of the disease. Normal tension glaucoma is usually detected after an examination of the optic nerve.
Those at higher risk for this form of glaucoma are people with
• family history of normal tension glaucoma
• Japanese ancestry
• Cardiovascular disease
(people with a history of systemic heart disease, such as irregular heart rhythm. In North America, normal tension glaucoma is more prevalent in women than in men)
The Glaucoma Research Foundation sponsored a collaborative international study to help determine the best treatment for this type of glaucoma. The study concluded that eye drops used to lower intraocular pressure were effective even in cases of normal tension glaucoma. Currently, most doctors treat normal tension glaucoma by keeping normal eye pressures as low as possible with medicines, laser surgery, or filtering surgery.
NTG is diagnosed by observing the optic nerve for signs of damage. This can be done in several ways. The doctor will look through the pupil and examine the shape and color of the optic nerve. A nerve that is cupped or is not a healthy pink color is a cause for concern.
Another advanced method is with an instrument that can give more detailed information about the 3-dimentional structure of the Optic Nerve cup -- the Heidelberg Retina Tomograph (HRT). The HRT uses a special laser to take 3-dimensional photographs of the optic nerve and surrounding retina. This laser, which is not powerful enough to harm the eye, is first focused on the surface of the optic nerve and captures that image. Then it is focused on the layer just below the surface and captures that image. The HRT continues to take images of deeper and deeper layers until the desired depth has been reached. Finally, the instrument takes all these pictures of the layers and puts them together to form a 3-dimentional image of the entire optic nerve. The HRT takes 32 layer-by-layer pictures from the surface of the optic nerve to from 0.5 mm to 4.0 mm deep into the ocular structures. The computer then piles all the slices together in a reconstructed paper printout that looks like a map drawn to represent the hills and valleys of a geographical area. By color coding areas of elevation and depression, the HRT provides a two-dimensional representation of what the original, three-dimensional, stack looks like.
Another procedure is the visual field test. This test produces a map of the patient’s complete field of vision. Using this test, the doctor can check for any areas of sight loss that may be caused by damage to the optic nerve. This would appear as slight changes in the person’s vision occurring anywhere from near the center to the edge of the field of vision. These changes are not necessarily noticeable to the patient.
4. Secondary Glaucoma
Glaucoma can occur as the result of an eye injury, inflammation, tumor or in advanced cases of cataract or diabetes. It can also be caused by certain drugs such as steroids. This form of glaucoma may be mild or severe. The type of treatment will depend on whether it is open-angle or angle-closure glaucoma.
- Pseudoexfoliative Glaucoma
This form of secondary open-angle glaucoma occurs when a flaky, dandruff-like material peels off the outer layer of the lens within the eye. The material collects in the angle between the cornea and iris and can clog the drainage system of the eye, causing eye pressure to rise. Pseudoexfoliative Glaucoma is common in those of Scandinavian descent. Treatment usually includes medications or surgery.
- Pigmentary Glaucoma
A form of secondary open-angle glaucoma, this occurs when the pigment granules in the back of the iris (the colored part of the eye) break into the clear fluid produced inside the eye. These tiny pigment granules flow toward the drainage canals in the eye and slowly clog them, causing eye pressure to rise. Treatment usually includes medications or surgery.
Although rare, pigment dispersion syndrome and pigmentary glaucoma tend to occur at a younger age than primary open-angle glaucoma. Pigment dispersion syndrome occurs when pigment granules that normally adhere to the back of the iris (the colored part of the eye), flake off into the clear fluid produced in the eye, called the aqueous humor. Sometimes these granules flow toward the drainage canals of the eye, slowly clogging them and raising eye pressure. This rise in eye pressure can damage the optic nerve, the nerve in the back of the eye that carries visual images to the brain. If this happens, pigment dispersion syndrome becomes pigmentary glaucoma.
Doctors usually treat pigmentary glaucoma with eyedrops such as Betagan, Timoptic, Optipranlol and Xalatan. These eyedrops have a relatively low incidence of side effects and are generally well-tolerated in younger patients. Doctors may also use medications such as Pilocar, and Ocusert, which are from a class of drugs called miotics. These medications cause the pupil to constrict (become smaller) and inhibit the iris from rubbing against the supporting fibers of the eye’s lens, helping to prevent further release of pigment. However, miotics have side effects such as blurred vision which can limit their use.
In some patients, a laser treatment called argon laser trabeculoplasty works well. This procedure helps open up the drainage system in the eye to increase fluid flow, which lowers eye pressure and protects the optic nerve.
Another treatment for pigmentary glaucoma is a procedure called a laser iridotomy. A laser is used to make a small hole in the iris, causing the iris to move away from the lens of the eye. This prevents the lens fibers from scraping the pigment from the iris and clogging the eye’s fluid flow. However, it has limitations and does not always achieve its desired effect. Researchers are now conducting more evaluations of this procedure to determine its effectiveness.
The Exercise Connection
Studies have found that vigorous exercise such as jogging and basketball can cause more pigment to be released from the iris, which can further block eye drainage. Patients with pigment dispersion syndrome or pigmentary glaucoma should discuss this issue with their doctor.
Progression of pigment dispersion syndrome into pigmentary glaucoma
It is estimated that pigment dispersion syndrome develops into pigmentary glaucoma in about 30% of cases. Although pigment dispersion syndrome appears to strike both men and women at an equal rate, researchers are investigating why men develop pigmentary glaucoma up to three times more often than women. Studies have also shown this syndrome develops into pigmentary glaucoma at a younger age in men than in women.
- Traumatic Glaucoma
Injury to the eye may cause secondary open-angle glaucoma. This type of glaucoma can occur immediately after the injury or years later. It can be caused by blunt injuries that “bruise” the eye (called blunt trauma) or by injuries that penetrate the eye. In addition, conditions such as severe nearsightedness, previous injury, infection, or prior surgery may make the eye more vulnerable to a serious eye injury.
- Neovascular Glaucoma
The abnormal formation of new blood vessels on the iris and over the eye’s drainage channels can cause a form of secondary open-angle glaucoma.
Neovascular glaucoma is always associated with other abnormalities, most often diabetes. It never occurs on its own. The new blood vessels block the eye’s fluid from exiting through the trabecular meshwork (the eye’s drainage canals), causing an increase in eye pressure. This type of glaucoma is very difficult to treat.
- Irido Corneal Endothelial Syndrome (ICE)
This rare form of glaucoma usually appears in only one eye, rather than both. Cells on the back surface of the cornea spread over the eye’s drainage tissue and across the surface of the iris, increasing eye pressure and damaging the optic nerve. These corneal cells also form adhesions that bind the iris to the cornea, further blocking the drainage channels.
Irido Corneal Endothelial Syndrome occurs more frequently in light-skinned females. Symptoms can include hazy vision upon awakening and the appearance of halos around lights. Treatment can include medications and filtering surgery. Laser therapy is not effective in these cases.
5. Pediatric or Childhood Glaucoma
The pediatric glaucomas consist of congenital glaucoma (present at birth), infantile glaucoma (appears during the first three years), juvenile glaucoma (age three through the teenage or young adult years), and all the secondary glaucomas occurring in the pediatric age group.
Congenital glaucoma is present at birth and most cases are diagnosed during the first year of life. Sometimes symptoms are not recognized until later in infancy or early childhood. The range of treatment is very different from that for adult glaucoma. It is very important to catch pediatric glaucoma early in order to prevent blindness. This is a rare condition that may be inherited, caused by incorrect development of the eye’s drainage system before birth. This leads to increased intraocular pressure, which in turn damages the optic nerve.
Childhood glaucoma occurs in one out of every 10,000 births in the United States. In most cases, childhood glaucoma is diagnosed by the age of six months, with 80 diagnosed by the first year of life. Up to 50 of hyphema (blunt trauma to the eyeball) patients are at risk of developing glaucoma. These traumas to the eye can include a variety of injuries — from walking into a twig to getting hit in the eye by a baseball.
Signs of Childhood Glaucoma under 2:
• Unusually large eyes
• Excessive tearing
• Cloudy cornea
• Photosensitivity (sensitivity to light)
Other signs and questions you may ask for all children under 18:
• Are your child’s eyes particularly sensitive to sunlight or a camera flash?
• Have you noticed significant vision loss in your child?
• Do your child’s eyes have difficulty adjusting in the dark?
• Does your child complain of headaches and/or eye pain?
• Does your child blink or/and squeeze his/her eyes often?
• Does your child have red eyes all the time?
Other conditions to be monitored:
• Any child with eye injury or a history of a serious eye injury.
• Any child who has had cataract surgery. (Up to 25 % of patients can develop glaucoma after the surgery)
It’s important to note that for children over the age of two, there are no apparent signs or symptoms until the late stages of glaucoma. Also, parents should understand that glaucoma in young children has specific signs that do not appear in older children with the disease. As always, one of the best lines of defense against glaucoma is a regular and complete eye exam. Remember, every individual’s condition varies and doctors and parents need to work together to accommodate each child’s needs.
- Treatments
In an uncomplicated case, surgery can often correct such structural defects. Both medication and surgery are required in some cases. Medical treatments may involve the use of topical eye drops and oral medications. These treatments help to either increase the exit of fluid from the eye or decrease the production of fluid inside the eye. Each results in lower eye pressure.
There are two main types of surgical treatments: filtering surgery and laser surgery. Filtering surgery (also known as micro surgery) involves the use of small surgical tools to create a drainage canal in the eye. In contrast, laser surgery uses a small but powerful beam of light to make a small opening in the eye tissue.
- What to Expect
Thousands of children with glaucoma can live full lives. This is the ultimate goal of glaucoma management. Although lost vision cannot be restored, it is possible to optimize each child’s remaining vision. Equally important is to encourage your child’s independence and participation in his or her own self-care.
PREVENTION OF GLAUCOMA
Zur Bearbeitung hier klicken
Diagnostic Tests Early detection, through regular and complete eye exams, is the key to protecting your vision from damage caused by glaucoma.
It is important to have your eyes examined regularly. Your eyes should be tested:
Common Tests for Glaucoma
- Tonometry
The tonometry test measures the inner pressure of the eye. Usually drops are used to numb the eye. Then the doctor or technician will use a special device that measures the eye’s pressure.
- Ophthalmoscopy
Ophthalmoscopy is used to examine the inside of the eye, especially the optic nerve. In a darkened room, the doctor will magnify your eye by using an ophthalmoscope (an instrument with a small light on the end). This helps the doctor look at the shape and color of the optic nerve.
If the pressure in the eye is not in the normal range, or if the optic nerve looks unusual, then one or two special glaucoma tests will be done. These two tests are called perimetry and gonioscopy.
- Perimetry
The perimetry test is also called a visual field test. During this test, you will be asked to look straight ahead and then indicate when a moving light passes your peripheral (or side) vision. This helps draw a “map” of your vision.
- Gonioscopy
Gonioscopy is a painless eye test that checks if the angle where the iris meets the cornea is open or closed, showing if either open-angle or closed angle glaucoma is present.
- Optic Nerve Computer Imaging
In recent years three new techniques of optic nerve imaging have become widely available. These are scanning laser polarimetry (GDx), confocal laser ophthalmoscopy (Heidelberg Retinal Tomography or HRT), and optical coherence tomography (OCT).
The GDx machine does not actually image the optic nerve but rather it measures the thickness of the nerve fiber layer on the retinal surface just before the fibers pass over the optic nerve margin to form the optic nerve. The HRT scans the retinal surface and optic nerve with a laser. It then constructs a topographic (3-D) image of the optic nerve including a contour outline of the optic cup. The nerve fiber layer thickness is also measured. The OCT instrument utilizes a technique called optical coherence tomography which creates images by use of special beams of light. The OCT machine can create a contour map of the optic nerve, optic cup and measure the retinal nerve fiber thickness. Over time all three of these machines can detect loss of optic nerve fibers.
Your intraocular eye pressure (IOP) is important to determining your risk for glaucoma. If you have high IOP, careful management of your eye pressure with medications can help prevent vision loss. Recent discoveries about the cornea, the clear part of the eye’s protective covering, are showing that corneal thickness is an important factor in accurately diagnosing eye pressure. In response to these findings, the Glaucoma Research Foundation has put together this brief guide to help you understand how your corneal thickness affects your risk for glaucoma, and what you can do to make sure your diagnosis is accurate.
- Corneal Thickness
In 2002, the five-year report of the Ocular Hypertension Study (OHTS) was released. The study’s goal was to determine if early intervention with pressure lowering medications could reduce the number of ocular hypertensive (OHT) patients that develop glaucoma. During the study, a critical discovery was made regarding corneal thickness and its role in intraocular eye pressure and glaucoma development.
Corneal thickness is important because it can mask an accurate reading of eye pressure, causing doctors to treat you for a condition that may not really exist or to treat you unnecessarily when are normal. Actual IOP may be underestimated in patients with thinner CCT, and overestimated in patients with thicker CCT. This may be important to your diagnosis; some people originally diagnosed with normal tension glaucoma may in fact be more accurately treated as having regular glaucoma; others diagnosed with ocular hypertension may be better treated as normal based on accurate CCT measurement. In light of this discovery, it is important to have your eyes checked regularly and to make sure your doctor takes your CCT into account for diagnosis.
A Thin Cornea—The Danger of Misreading Eye Pressure
Many times, patients with thin corneas (less than 555 µm) show artificially low IOP readings. This is dangerous because if your actual IOP is higher than your reading shows, you may be at risk for developing glaucoma and your doctor may not know it. Left untreated, high IOP can lead to glaucoma and vision loss. It is important that your doctor have an accurate IOP reading to diagnose your risk and decide upon a treatment plan.
A Thicker Cornea May Mean Less Reason to Worry About Glaucoma
Those patients with thicker CCT may show a higher reading of IOP than actually exists. This means their eye pressure is lower than thought, a lower IOP means that risk for developing glaucoma is lowered. However, it is still important to have regular eye exams to monitor eye pressure and stay aware of changes.
Pachymetry—A Simple Test to Determine Corneal Thickness
A pachymetry test is a simple, quick, painless test to measure the thickness of your cornea. With this measurement, your doctor can better understand your IOP reading, and develop a treatment plan that is right for your condition. The procedure takes only about a minute to measure both eyes.
It is important to have your eyes examined regularly. Your eyes should be tested:
- before age 40, every two to four years
- from age 40 to age 54, every one to three years
- from age 55 to 64, every one to two years
- after age 65, every six to 12 months
Common Tests for Glaucoma
- Tonometry
The tonometry test measures the inner pressure of the eye. Usually drops are used to numb the eye. Then the doctor or technician will use a special device that measures the eye’s pressure.
- Ophthalmoscopy
Ophthalmoscopy is used to examine the inside of the eye, especially the optic nerve. In a darkened room, the doctor will magnify your eye by using an ophthalmoscope (an instrument with a small light on the end). This helps the doctor look at the shape and color of the optic nerve.
If the pressure in the eye is not in the normal range, or if the optic nerve looks unusual, then one or two special glaucoma tests will be done. These two tests are called perimetry and gonioscopy.
- Perimetry
The perimetry test is also called a visual field test. During this test, you will be asked to look straight ahead and then indicate when a moving light passes your peripheral (or side) vision. This helps draw a “map” of your vision.
- Gonioscopy
Gonioscopy is a painless eye test that checks if the angle where the iris meets the cornea is open or closed, showing if either open-angle or closed angle glaucoma is present.
- Optic Nerve Computer Imaging
In recent years three new techniques of optic nerve imaging have become widely available. These are scanning laser polarimetry (GDx), confocal laser ophthalmoscopy (Heidelberg Retinal Tomography or HRT), and optical coherence tomography (OCT).
The GDx machine does not actually image the optic nerve but rather it measures the thickness of the nerve fiber layer on the retinal surface just before the fibers pass over the optic nerve margin to form the optic nerve. The HRT scans the retinal surface and optic nerve with a laser. It then constructs a topographic (3-D) image of the optic nerve including a contour outline of the optic cup. The nerve fiber layer thickness is also measured. The OCT instrument utilizes a technique called optical coherence tomography which creates images by use of special beams of light. The OCT machine can create a contour map of the optic nerve, optic cup and measure the retinal nerve fiber thickness. Over time all three of these machines can detect loss of optic nerve fibers.
Your intraocular eye pressure (IOP) is important to determining your risk for glaucoma. If you have high IOP, careful management of your eye pressure with medications can help prevent vision loss. Recent discoveries about the cornea, the clear part of the eye’s protective covering, are showing that corneal thickness is an important factor in accurately diagnosing eye pressure. In response to these findings, the Glaucoma Research Foundation has put together this brief guide to help you understand how your corneal thickness affects your risk for glaucoma, and what you can do to make sure your diagnosis is accurate.
- Corneal Thickness
In 2002, the five-year report of the Ocular Hypertension Study (OHTS) was released. The study’s goal was to determine if early intervention with pressure lowering medications could reduce the number of ocular hypertensive (OHT) patients that develop glaucoma. During the study, a critical discovery was made regarding corneal thickness and its role in intraocular eye pressure and glaucoma development.
Corneal thickness is important because it can mask an accurate reading of eye pressure, causing doctors to treat you for a condition that may not really exist or to treat you unnecessarily when are normal. Actual IOP may be underestimated in patients with thinner CCT, and overestimated in patients with thicker CCT. This may be important to your diagnosis; some people originally diagnosed with normal tension glaucoma may in fact be more accurately treated as having regular glaucoma; others diagnosed with ocular hypertension may be better treated as normal based on accurate CCT measurement. In light of this discovery, it is important to have your eyes checked regularly and to make sure your doctor takes your CCT into account for diagnosis.
A Thin Cornea—The Danger of Misreading Eye Pressure
Many times, patients with thin corneas (less than 555 µm) show artificially low IOP readings. This is dangerous because if your actual IOP is higher than your reading shows, you may be at risk for developing glaucoma and your doctor may not know it. Left untreated, high IOP can lead to glaucoma and vision loss. It is important that your doctor have an accurate IOP reading to diagnose your risk and decide upon a treatment plan.
A Thicker Cornea May Mean Less Reason to Worry About Glaucoma
Those patients with thicker CCT may show a higher reading of IOP than actually exists. This means their eye pressure is lower than thought, a lower IOP means that risk for developing glaucoma is lowered. However, it is still important to have regular eye exams to monitor eye pressure and stay aware of changes.
Pachymetry—A Simple Test to Determine Corneal Thickness
A pachymetry test is a simple, quick, painless test to measure the thickness of your cornea. With this measurement, your doctor can better understand your IOP reading, and develop a treatment plan that is right for your condition. The procedure takes only about a minute to measure both eyes.