
Eye Disease Simulations

 |
 |
 |
 |
 |
 |
|
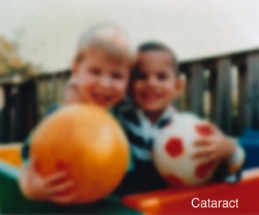
Cataract
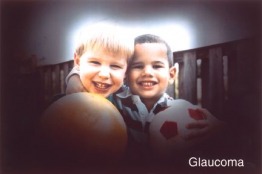
Conjunctival and Scleral Disorders Allergic Conjunctivitis Episcleritis Infectious Conjunctivitis Noncancerous Growths Scleritis Trachoma Corneal Disorders Bullous Keratopathy Corneal Ulcer Herpes Simplex Keratitis Herpes Zoster Ophthalmicus Keratoconjunctivitis Sicca Keratoconus Keratomalacia Peripheral Ulcerative Keratitis Superficial Punctate Keratitis Eyelid and Tearing Disorders Blepharitis Canaliculitis Chalazion Dacryocystitis Dacryostenosis Entropion and Ectropion Eyelid Tumors Stye (Hordeolum) Trichiasis Eye Socket Disorders Infections of the Orbit Preseptal cellulitis Orbital Cellulitis Inflammation of the Orbit Proptosis Tumors of the Orbit Glaucoma |
Injuries to the Eye
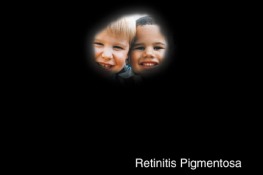
Blunt Injuries to the Eye Black Eye Subconjunctival Hemorrhage Hyphema Retinal Detachment Other Blunt Injuries to the Eyeball Chemical Burns to the Eye Corneal Abrasions and Foreign Bodies Eyelid Lacerations Fractures of the Orbit Lacerated Eyeball Traumatic Iritis and Chemical Iritis Optic Nerve Disorders Ischemic Optic Neuropathy Optic Neuritis Papilledema Toxic Amblyopia (Nutritional Amblyopia) Refractive Disorders Corrective Lenses Surgery for Refractive Errors Retinal Disorders Age-Related Macular Degeneration Blockage of Central Retinal Arteries and Veins Cancers Affecting the Retina Detachment of the Retina Diabetic Retinopathy Endophthalmitis Epiretinal Membrane Hypertensive Retinopathy Retinitis Pigmentosa Uveitis |
Flashes and Floaters
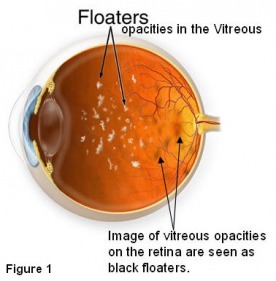
Floaters are entoptic images of opacities in the vitreous (Figure 1). Entoptic image is a visual perception that is produced by structures within the eye - in this case vitreous opacities. Patients complain of small specks or dots that can be seen against a bright background such as a diffusely illuminated wall or the blue sky. Sometimes fine dark lines in amorphous mass - like small branching twigs - are seen. These floaters move around and are also called 'muscae volitantes' because they seem to dart about like flies as the eye is moved. Over time you will become less aware of these floaters as the brain learns to ignore these retinal images. Therefore, while some floaters may remain in your vision, many of them will fade over time and become less bothersome.
Floaters are entoptic images of opacities in the vitreous (Figure 1). Entoptic image is a visual perception that is produced by structures within the eye - in this case vitreous opacities. Patients complain of small specks or dots that can be seen against a bright background such as a diffusely illuminated wall or the blue sky. Sometimes fine dark lines in amorphous mass - like small branching twigs - are seen. These floaters move around and are also called 'muscae volitantes' because they seem to dart about like flies as the eye is moved. Over time you will become less aware of these floaters as the brain learns to ignore these retinal images. Therefore, while some floaters may remain in your vision, many of them will fade over time and become less bothersome.
 |
 |
 |
 |
 |
 |
Floaters, if present since a long time or increasing in number very gradually, are harmless. They may be annoying but do not cause any problems. However if a new floater comes on abruptly or if there is a sudden increase in the number of floaters, then you must be examined immediately to rule out a retinal tear.
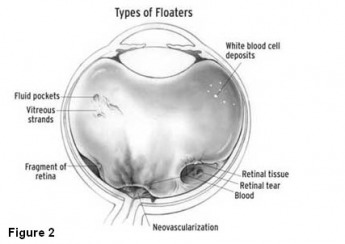
Floaters may be due condensations of vitreous collagen (single or clumped hair-like floaters formed in degenerating/liquefying vitreous as occurs with aging) or due to blood (abrupt shower of small floaters usually from retinal tear), or glial tissue torn from an area adjacent to the optic nerve head (abrupt single or few large floaters, occurs in posterior vitreous detachment). A dilated fundus examination should be immediately performed for any abrupt increase in the number of floaters.
The vitreous gel is 99% water and 1% solid elements. Of the solid portion, there are collagen filaments and hyaluronic acid molecules. The ability of hyaluronic acid molecules to retain water molecules is an important factor in maintaining the gel consistency of vitreous. With age, there is a depolymerisation of hyaluronic acid, causing these molecules to release their water and form lacunae i.e. pockets of liquefied vitreous. The collagen 'filaments' aggregate to form larger 'fibrils', causing further collapse of the vitreous gel structure. This process is known as vitreous degeneration and 'syneresis'. The collagen fibrils may 'float' within the liquid vitreous pockets, giving the patient a sensation of floaters. The same process that causes floaters may cause flashes of light. When the vitreous pulls on the retina - to which it is attached - the photoreceptors are mechanically stimulated. The retinal cells are incapable of perceiving pain, pressure, or temperature. The only stimulus that the retina responds to is 'light'. So when the retinal photoreceptors experience mechanical stimulation because of the vitreous pull, they send a signal to the brain in the form of disorganized light, which is perceived by the brain as a 'flash'.
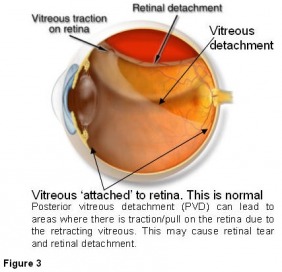
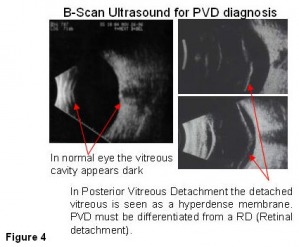
Eventually, with the accumulation of enough lacunae (liquified vitreous pockets), the vitreous framework collapses and the vitreous completely separates from the retina. This process is called posterior vitreous detachment (Figure 3). Tissue may tear from an area adjacent to or from the optic nerve head due to an acute posterior vitreous detachment. This tissue (called Weiss ring) is usually visible as a large floater. Posterior vitreous detachment occurs in less that 10% people under 50 years of age but in more than 60% people who are over 70 years of age. It is more common for people who are nearsighted or who have had an eye injury or have undergone eye surgery or who have had inflammation inside the eye. B-scan ultrasound (Figure 4) examination is the only method that can definitively diagnose posterior vitreous detachment.
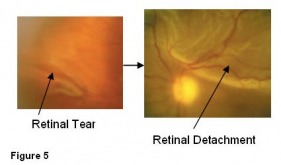
The reason why you are advised not to ignore symptoms of sudden increase in the number of floaters or flashes of light especially if accompanied by subjective reduction in vision (cloud or curtain in vision) is that these symptoms signify an acute posterior vitreous detachment. There could be an associated retinal tear which can lead to a retinal detachment (Figure 5). Therefore you should have an immediate eye examination to rule out any retinal involvement. A dilated fundus examination is required. Another examination will be performed after 4 to 6 weeks if the first examination is normal.
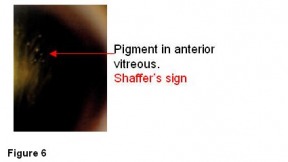
Approximately 15% patients with acute symptomatic posterior vitreous detachment (sudden increase in flashes, floaters or subjective vision reduction) have retinal tears. If there is an associated vitreous hemorrhage then the likelihood of finding a retinal hole increases to 70%. Another sign that increases the likelihood of finding a retinal tear is the presence of pigment in the anterior vitreous (called Shaffer’s sign (Figure 6) on slit lamp examination). Patients with posterior vitreous detachment with vitreous pigment granules or hemorrhage are 52 times more likely to have a retinal tear compared with those who have normal findings on vitreous examination
While most floaters reside in the vitreous gel, it is important not to overlook another simpler reason - namely, debris in the tear film. It is not uncommon for patients to accumulate make-up or other material within their tears. Patients with blepharitis and meibomian gland dysfunction may also accumulate debris within the tear layer, which can be reported as floaters. This phenomenon is transient and the patient may report that the floaters move significantly upon blinking. Patients with ocular allergies may also report this phenomenon, since their eyes produce excess mucus. These mucus strands can float over the pupil area and simulate floaters. The key to their differentiation from vitreous floaters is the observation of excessive movement or even disappearance of tear film debris floaters with blinking only - without eye movement. Vitreous floaters typically will move more with eye movements than with blinking.
Treatment of Vitreous floaters
Standard vision tests like the Snellen visual acuity measurement, which quantifies your vision as 20/20 etc are unable to quantify many aspects of a visual disability due to floaters and how the disability interferes with day-to-day functioning and overall quality of life. Responses to subjective questionnaires may be more indicative of visual dysfunction. In some patients floaters can cause persistent, distracting and disabling symptoms. In these patients, visual tasks such as reading or driving become laborious, and productivity and overall quality of life may suffer. It is advisable to wait at least one year to allow enough time for the floaters to become less prominent naturally. If they do not, then one can consider laser surgery or vitrectomy surgery.
We must caution at the very outset of this discussion that laser or surgical treatment of floaters is not considered a standard management strategy or algorithm and is recommended by a minority of physicians, even then under exceptional circumstances. We are not aware of any vitamins or drugs that can reduce floaters.
Vitrectomy
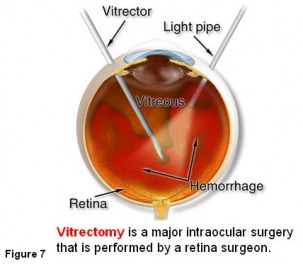
Pars plana vitrectomy (PPV) Figure 7 is a procedure usually reserved for complicated posterior segment disease. It has a well-known risk profile and justifiably there is reluctance to offer this surgery to treat floaters. However the post-operative complication rate following PPV has been assessed in the setting of retinal detachment surgery or in the presence of complicated vitreo-retinal disease. It may be argued that pars plana vitrectomy for floaters, in eyes that have an established posterior vitreous detachment (PVD), may be associated with a lower incidence of both intraoperative and post-operative complications. The three main postoperative complications that one must worry about in vitrectomy are: development or progression of nuclear sclerosis cataract, retinal detachment and choroidal or vitreous hemorrhage (bleeding) in the eye.
Pars plana vitrectomy has been reported to be a highly effective treatment for floaters with complete resolution of symptoms recorded in about 90% of patients in some studies. (Eye 2002; 16,:21-26; Retina 2000;20:591-6).
Laser Surgery
A Nd:YAG laser is used to 'disrupt' the floaters. The laser places a high energy acoustic (sound-wave) pulse close to the floater. This energy pulse disrupts/blasts the floater. Technically this procedure is termed 'vitriolysis'. Despite studies describing laser vitreolysis as a treatment for vitreous floaters, this technique is not widely practiced. The reason for this may be a combination of disappointing results, or reluctance to use Nd:YAG laser in the posterior segment of the eye. The latter may be influenced by the known complication of retinal detachment following YAG laser capsulotomy (performed after a cataract surgery), which occurs at an incidence of between 0.50% and 4.16%.
A recent study showed that laser surgery for floaters ameliorated symptoms in only a third of patients. Furthermore the clinical improvement was only moderate in degree, subjectively being graded at no greater than 50% by 93.3% of patients. In no patient was there complete resolution of symptoms. Laser treatment led to worsening of symptoms in 7.7% of patients (Eye 2002; 16,:21-26).
Migraines may also cause flashes
Migraines are more prevalent in the 25 to 44 years age group, with females being affected 2.5 times more frequently than males. Classic migraine has three distinct phases: a prodromal phase, a headache phase, and a resolution phase. Several visual symptoms appear during the prodromal phase of migraine.
The most common visual aura in the prodromal phase is the scintillating scotoma. 'Scintillating' means 'sparkling flashes' and 'scotoma' means 'a non-seeing area'. It usually begins as a shimmering arc of white or colored lights. The arc of light gradually enlarges, becomes more obvious, and may take the form of a definite zig-zag pattern. On occasion, this is preceded or followed by a spreading zone of visual loss. Even if there is no identifiable area of visual loss, the disturbance of vision created by the scintillating scotoma may make reading and driving difficult. Scintillating scotoma may also be accompanied by mild feelings of dizziness or vertigo. The zig-zag appearance may become so pronounced that the term "fortification spectrum" may be applied because of the resemblance to the ground plans of a fort (view the scintillating scotoma animation). Sometimes the visual symptoms appear as a "ball of light" in the center of the visual fields which obscures vision to a great degree. These visual phenomenon may last 20 to 30 minutes.
Migraine flashes are usually caused by a spasm of blood vessels in the brain. If a headache follows the flashes, it is called a migraine headache. However, visual phenomenon can occur without a headache. In this case, the light flashes are called ophthalmic migraine, or migraine without headache.
Floaters may be due condensations of vitreous collagen (single or clumped hair-like floaters formed in degenerating/liquefying vitreous as occurs with aging) or due to blood (abrupt shower of small floaters usually from retinal tear), or glial tissue torn from an area adjacent to the optic nerve head (abrupt single or few large floaters, occurs in posterior vitreous detachment). A dilated fundus examination should be immediately performed for any abrupt increase in the number of floaters.
The vitreous gel is 99% water and 1% solid elements. Of the solid portion, there are collagen filaments and hyaluronic acid molecules. The ability of hyaluronic acid molecules to retain water molecules is an important factor in maintaining the gel consistency of vitreous. With age, there is a depolymerisation of hyaluronic acid, causing these molecules to release their water and form lacunae i.e. pockets of liquefied vitreous. The collagen 'filaments' aggregate to form larger 'fibrils', causing further collapse of the vitreous gel structure. This process is known as vitreous degeneration and 'syneresis'. The collagen fibrils may 'float' within the liquid vitreous pockets, giving the patient a sensation of floaters. The same process that causes floaters may cause flashes of light. When the vitreous pulls on the retina - to which it is attached - the photoreceptors are mechanically stimulated. The retinal cells are incapable of perceiving pain, pressure, or temperature. The only stimulus that the retina responds to is 'light'. So when the retinal photoreceptors experience mechanical stimulation because of the vitreous pull, they send a signal to the brain in the form of disorganized light, which is perceived by the brain as a 'flash'.
Eventually, with the accumulation of enough lacunae (liquified vitreous pockets), the vitreous framework collapses and the vitreous completely separates from the retina. This process is called posterior vitreous detachment (Figure 3). Tissue may tear from an area adjacent to or from the optic nerve head due to an acute posterior vitreous detachment. This tissue (called Weiss ring) is usually visible as a large floater. Posterior vitreous detachment occurs in less that 10% people under 50 years of age but in more than 60% people who are over 70 years of age. It is more common for people who are nearsighted or who have had an eye injury or have undergone eye surgery or who have had inflammation inside the eye. B-scan ultrasound (Figure 4) examination is the only method that can definitively diagnose posterior vitreous detachment.
The reason why you are advised not to ignore symptoms of sudden increase in the number of floaters or flashes of light especially if accompanied by subjective reduction in vision (cloud or curtain in vision) is that these symptoms signify an acute posterior vitreous detachment. There could be an associated retinal tear which can lead to a retinal detachment (Figure 5). Therefore you should have an immediate eye examination to rule out any retinal involvement. A dilated fundus examination is required. Another examination will be performed after 4 to 6 weeks if the first examination is normal.
Approximately 15% patients with acute symptomatic posterior vitreous detachment (sudden increase in flashes, floaters or subjective vision reduction) have retinal tears. If there is an associated vitreous hemorrhage then the likelihood of finding a retinal hole increases to 70%. Another sign that increases the likelihood of finding a retinal tear is the presence of pigment in the anterior vitreous (called Shaffer’s sign (Figure 6) on slit lamp examination). Patients with posterior vitreous detachment with vitreous pigment granules or hemorrhage are 52 times more likely to have a retinal tear compared with those who have normal findings on vitreous examination
While most floaters reside in the vitreous gel, it is important not to overlook another simpler reason - namely, debris in the tear film. It is not uncommon for patients to accumulate make-up or other material within their tears. Patients with blepharitis and meibomian gland dysfunction may also accumulate debris within the tear layer, which can be reported as floaters. This phenomenon is transient and the patient may report that the floaters move significantly upon blinking. Patients with ocular allergies may also report this phenomenon, since their eyes produce excess mucus. These mucus strands can float over the pupil area and simulate floaters. The key to their differentiation from vitreous floaters is the observation of excessive movement or even disappearance of tear film debris floaters with blinking only - without eye movement. Vitreous floaters typically will move more with eye movements than with blinking.
Treatment of Vitreous floaters
Standard vision tests like the Snellen visual acuity measurement, which quantifies your vision as 20/20 etc are unable to quantify many aspects of a visual disability due to floaters and how the disability interferes with day-to-day functioning and overall quality of life. Responses to subjective questionnaires may be more indicative of visual dysfunction. In some patients floaters can cause persistent, distracting and disabling symptoms. In these patients, visual tasks such as reading or driving become laborious, and productivity and overall quality of life may suffer. It is advisable to wait at least one year to allow enough time for the floaters to become less prominent naturally. If they do not, then one can consider laser surgery or vitrectomy surgery.
We must caution at the very outset of this discussion that laser or surgical treatment of floaters is not considered a standard management strategy or algorithm and is recommended by a minority of physicians, even then under exceptional circumstances. We are not aware of any vitamins or drugs that can reduce floaters.
Vitrectomy
Pars plana vitrectomy (PPV) Figure 7 is a procedure usually reserved for complicated posterior segment disease. It has a well-known risk profile and justifiably there is reluctance to offer this surgery to treat floaters. However the post-operative complication rate following PPV has been assessed in the setting of retinal detachment surgery or in the presence of complicated vitreo-retinal disease. It may be argued that pars plana vitrectomy for floaters, in eyes that have an established posterior vitreous detachment (PVD), may be associated with a lower incidence of both intraoperative and post-operative complications. The three main postoperative complications that one must worry about in vitrectomy are: development or progression of nuclear sclerosis cataract, retinal detachment and choroidal or vitreous hemorrhage (bleeding) in the eye.
Pars plana vitrectomy has been reported to be a highly effective treatment for floaters with complete resolution of symptoms recorded in about 90% of patients in some studies. (Eye 2002; 16,:21-26; Retina 2000;20:591-6).
Laser Surgery
A Nd:YAG laser is used to 'disrupt' the floaters. The laser places a high energy acoustic (sound-wave) pulse close to the floater. This energy pulse disrupts/blasts the floater. Technically this procedure is termed 'vitriolysis'. Despite studies describing laser vitreolysis as a treatment for vitreous floaters, this technique is not widely practiced. The reason for this may be a combination of disappointing results, or reluctance to use Nd:YAG laser in the posterior segment of the eye. The latter may be influenced by the known complication of retinal detachment following YAG laser capsulotomy (performed after a cataract surgery), which occurs at an incidence of between 0.50% and 4.16%.
A recent study showed that laser surgery for floaters ameliorated symptoms in only a third of patients. Furthermore the clinical improvement was only moderate in degree, subjectively being graded at no greater than 50% by 93.3% of patients. In no patient was there complete resolution of symptoms. Laser treatment led to worsening of symptoms in 7.7% of patients (Eye 2002; 16,:21-26).
Migraines may also cause flashes
Migraines are more prevalent in the 25 to 44 years age group, with females being affected 2.5 times more frequently than males. Classic migraine has three distinct phases: a prodromal phase, a headache phase, and a resolution phase. Several visual symptoms appear during the prodromal phase of migraine.
The most common visual aura in the prodromal phase is the scintillating scotoma. 'Scintillating' means 'sparkling flashes' and 'scotoma' means 'a non-seeing area'. It usually begins as a shimmering arc of white or colored lights. The arc of light gradually enlarges, becomes more obvious, and may take the form of a definite zig-zag pattern. On occasion, this is preceded or followed by a spreading zone of visual loss. Even if there is no identifiable area of visual loss, the disturbance of vision created by the scintillating scotoma may make reading and driving difficult. Scintillating scotoma may also be accompanied by mild feelings of dizziness or vertigo. The zig-zag appearance may become so pronounced that the term "fortification spectrum" may be applied because of the resemblance to the ground plans of a fort (view the scintillating scotoma animation). Sometimes the visual symptoms appear as a "ball of light" in the center of the visual fields which obscures vision to a great degree. These visual phenomenon may last 20 to 30 minutes.
Migraine flashes are usually caused by a spasm of blood vessels in the brain. If a headache follows the flashes, it is called a migraine headache. However, visual phenomenon can occur without a headache. In this case, the light flashes are called ophthalmic migraine, or migraine without headache.